The Wrist Joint complex said to the interconnected structures that allow for the wide range of motion and functionality in the wrist. It includes multiple bones, joints, ligaments, and other soft tissues.
The Wrist Joint.
Table of Contents
The bones which are involved in Wrist Joint-
Distal Radius and Ulna (forearm bones)
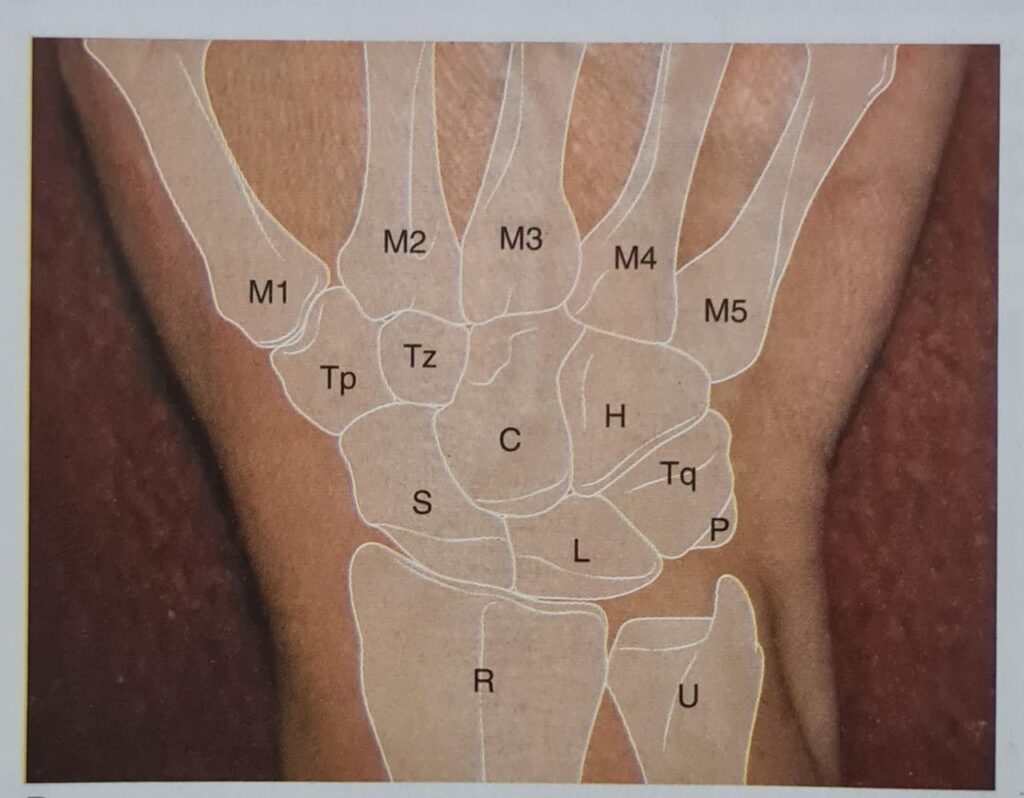
Carpal Bones (8 small bones arranged in two rows):
Proximal row: Scaphoid, Lunate, Triquetrum, Pisiform.
Distal row: Trapezium, Trapezoid, Capitate, Hamate.
- Movement of the Radiocarpal and Midcarpal Joints. Movements are caused by combination of active muscular and passive ligamentous and joint reaction forces
- Although there are abundant passive forces on the proximal carpal row, no muscular forces are applied directly to the articular bones of the proximal row, given that the flexor carpi ulnaris muscle applies its force via the pisiform to the more distal bones.
- The proximal carpals, therefore, are effectively a mechanical link that lies between the radius and the distal carpals and metacarpals, to which the muscular forces are actually applied.
- The proximal carpal row functions as an intercalated segment between the distal radius/triangular fibrocartilage complex and the relatively less mobile distal carpal row.
- When compressive forces are applied across an intercalated segment, the middle segment tends to collapse and move in the opposite direction from the segments above and below.
- An intercalated segment requires some type of stabilizing mechanism to normalize combined midcarpal/radiocarpal motion and prevent collapse of the middle segment (the proximal carpal row).
- The stabilization mechanism appears to involve the scaphoid’s functional and anatomical (ligamentous) connections to the adjacent lunate and to the distal carpal row.
Garcia-Elias supported the hypothesis that the stability of the proximal carpal row depends on the interaction of two opposite tendencies when the carpals are axially loaded (compressed across a neutral wrist); the scaphoid tends to flex, whereas the lunate and triquetrum tend to extend. These opposite rotations within the proximal row are prevented by the ligamentous structure, including the key scapholunate interosseous and lunotriquetral interosseous ligaments.
Keystone Of The Wrist Joint
- Much of the literature proposes that the head of the capitate, frequently referred to as the keystone of the wrist.
- May serve as the location of the coronal axis for wrist extension/flexion and the anteroposterior (A-P) axis for radial/ulnar deviation, as well as providing the rigid center of the fixed carpal arch.
FLEXION/EXTENSION OF THE WRIST JOINT
- During flexion/extension of the wrist, the scaphoid seems to show the greatest motion of the three proximal carpal bones, whereas the lunate moves least.
- Active extension is initiated at the distal carpal row attached metacarpals by the extensor muscles OF THE Wrist which attached to those bones. The distal carpals such as capitate, hamate, trapezium, and trapezoid) glide on the proximal row that are scaphoid, lunate, and triquetrum.
- Continued extensor force results in movement of the combined distal carpal row and the scaphoid bone on the fixed lunate and triquetrum at approximately 45° of extension of the wrist Joint complex, the scapholunate interosseous ligament brings the scaphoid and lunate into close-packed position. This unites all the carpals and causes them to function in the next phase as a single unit.
- Wrist motion from full extension to full flexion occurs in the reverse sequence. In the context of this conceptual frame-work, the scaphoid through mediation of the wrist ligaments.
- As wrist extension is initiated from full flexion then the distal carpal row moves on the proximal carpal row until neutral flexion/extension.
- The scaphoid and distal row move on the lunate/triquetrum from neutral to 45° of extension.
- The carpals move as a unit on the radius and triangular fibrocartilage complex to achieve the full wrist extension.
Instability of the Wrist Joint
- Injury any of the ligaments attached to the scaphoid and lunate bone may result in the reduction synergistic stabilization of the lunate and scaphoid. When this happens then the scaphoid bone act as an unconstrained segment and follows its natural tendency to collapse into flexion on the volarly inclined surface of the distal radius.
- The base of the flexed scaphoid slides dorsally on the radius and may subluxate. Once released from ligamentous stabilization with the scaphoid, both the lunate and triquetrum together act as an unconstrained segment, following their natural tendency to extend (rotate dorsally).
- The muscles applying forces to the distal carpals (none act on the proximal carpals) cause the distal carpals to flex on the extended lunate and triquetrum. The flexed distal carpals glide dorsally on the lunate and triquetrum. This zigzag pattern of the three segments (the scaphoid, the lunate,triquetrum and the distal carpal row is called as intercalated segmental instability.
When the lunate assumes an extended posture, the presentation is referred to as dorsal intercalated segmental instability (DISI). - When the scaphoid bone subluxate leads to compressive loading of the Wrist Joint along with the forces of the muscles.
- Subluxation of the scaphoid bone the pressure between the radius and scaphoid increase because of the contact occurs over a smaller area. Due to instability of the Dorsal Intercalated segmental Instability it start to show degenerative changes at the radio-scaphoid joint and other intercarpal joints.
- The progressive degenerative problem from an untreated dorsal intercalated segmental instability is known as scapholunate advanced collapse (SLAC) wrist.
- The lesser tendency toward degenerative changes in the radio-lunate joint has been attributed to a more spherical configuration of the radio-lunate facets that better center applied loads across the articular surfaces.
- The other common form of carpal instability occurs when the ligamentous union of the lunate and triquetrum is disrupted through injury.
- When the lunate is no longer linked with the triquetrum, then the lunate and scaphoid bone together fall into flexion and the triquetrum and distal row is extend. This ulnar and lunate instability is called as volar intercalated segmental instability (VISI).
Function Of The Wrist Joint
The hand consists of five digits: four fingers and a thumb. Each digit has a carpometacarpal joint and a metacarpophalangeal (MP) joint, each fingers have two interphalangeal (IP) joints-the proximal interphalangeal (PIP) and the and the distal interphalangeal (DIP) joints.
The thumb has one interphalangeal joint. Although the joints of the fingers and the joints of the thumb are same in structural but different in functions.
Palmar Arch of the hand
- The palmar arches allow the palm and the digits to conform optimally to the shape of the object being held, this helps to maximize the amount of surface contact and enhance the stability while increasing sensory feedback.
- The function of the finger carpometacarpal joints and their segments overall is to contribute with the thumb to the palmar arch system.
- The adjustable positions of the first, fourth, and fifth metacarpal heads around the relatively fixed second and third metacarpals form a mobile distal transverse arch at the level of the metacarpal heads that augments the fixed proximal transverse arch of the distal carpal row.
Volar Plates of the hand
- The volar plate also knowns as Palmar plate, present at each of the metacarpophalangeal joints is structure that increases joint congruency.
- It also provides stability to the metacarpophalangeal joint by limiting hyperextension and also provide support to the longitudinal arch.
Types of Power Grips
The fingers in power grip usually function is to hold an object in the palm. The fingers assume a position and manages flexion that varies in degree with the size, shape, and weight of the object where as the thumb serve as an additional surface to the finger-palm for better stability. This is in contrast to precision handling in which the thumb is more likely to be abducted.
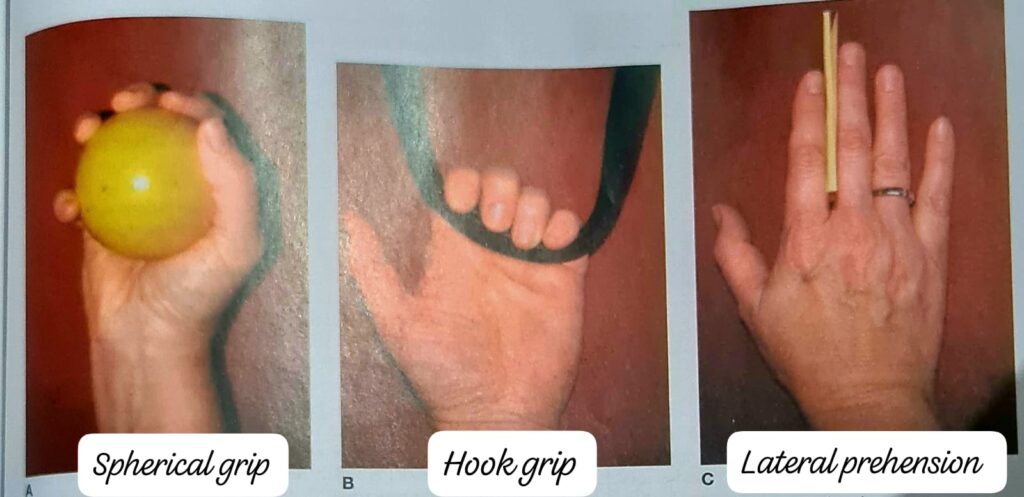
Four types of power grips are as follows:-
- Spherical Grip:- The extrinsic finger, the thumb flexors and the thenar muscles follow similar patterns of activity and variability. The main distinction can be made by the greater spread of the fingers to encompass the object. This evokes more interosseous activity than is seen in other forms of power grip. The phalanges are no longer parallel to each other, as they commonly are in cylindrical grip. The metacarpophalangeal joint abductors must be joined by the adductors to stabilize the joints.
- Hook Grip:- It may include the palm but never includes the thumb. It can be sustained for prolonged periods of time for example-a person who has carried a briefcase hung onto a commuter strap on a bus or train. The major muscular activity is provided by the flexor digitorum profundus and flexor digitorum superficialis muscles.
- Cylindrical Grip:- It is a one of the powerful grip of the hand uses the muscle name Extrinsic finger flexor to position the finger and maintain the powerful grasping of any object. The main muscle which helps to enhance the cylindrical grip is Flexor digitorum profundus. The muscle name Hypothenar is actively participate in this grip. This grip performed when the wrist joint is in neutral flexion or extension and slightly ulnar deviated.
- Lateral Prehension:- It is a unique form of grasping any thin object like Cards or cigarettes in which contact between two adjacent fingers is required to hold the objects but is not a powerful grip. The metacarpophalangeal and interphalangeal joints are usually maintained in extension This is the only form of prehension in which the finger extensor musculature predominates in the maintenance of the posture. Lateral prehension is included a form of power grip because lateral prehension involves the static holding of an object that is then moved by the more proximal joints of the upper extremity.
To learn and understand more about Ultrasound Therapy click the link given- https://physiocontent.com/ultraviolet-radiation-therapy-and-its-physiological-effects/
To learn and understand more about Human Spine click the link given- https://physiocontent.com/human-spine-backbone/